
2. Introducing the final search assignment.
Objectives:
After going over the content of this chapter and the linked video, students will:
1. be aware of the topic assigned for the final search assignment and the topic that will be used for the search demonstrations in these chapters.
2. be familiar with the disease and drugs that are central to the searches.
3. have outlined the major search concepts in the “demonstration” and “final search assignment” searches.
4. be aware of the requirements and deadlines for the final search assignment.
Objective 1. Students will be aware of the topic assigned for the final search assignment and the topic that will be used for the search demonstrations in these chapters.
I will demonstrate the creation of comprehensive search strategies in the coming chapters. These “demonstration” searches will identify journal articles that addresses the question:
- Does the available evidence support the use of omacetaxine in bcr-abl+ chronic myelogenous leukemia (CML)?
You will compose your “final search assignment” searches piece by piece as you work on lab assignments. Your “final search assignment” searches will identify journal articles that address the question:
- Does the available evidence support the efficacy of nilotinib in treatment of bcr-abl+, chronic myelogenous leukemia (CML) that is resistant to another anti-cancer drug?
The “demonstration” and “final search assignment” searches share the CML concept. You may copy the CML portion of the search from the demonstrations in this course book. You will still have a lot of search work to complete independently ( or with fellow students) as the “final search assignment” search concerns resistant forms of CML and a different drug.
Objective 2. Students will be familiar with the disease and drugs that are central to the searches.
When designing a search strategy, it’s very helpful to know a bit about the search concepts. So this chapter will introduce you to the concepts included in the “demonstration” and “final search assignment” searches.
After you read this section and watch the included video, you should:
-
- be familiar with the microscopic appearance of the blood in patients with chronic myelogenous leukemia (CML), the symptoms of CML, and the three phases of CML
- be familiar with the genetic defect that causes CML and the treatments targeted at that defect.
- be aware that some patients are resistant to, or become resistant to, CML treatments.
Chronic Myelogenous Leukemia (CML)
Please, watch the first 11 minutes of the following video. The video was produced by the Leukemia & Lymphoma Society. It provides basic information about CML while introducing you to CML patients, doctors and scientists who have been fighting the disease. Specifically, the video shows how a chromosomal translocation (Philadelphia chromosome) produces the bcr-abl gene that causes CML, discusses the revolutionary design of the tyrosine kinase inhibitor drugs that target the protein product of the bcr-abl gene, and discusses the plight faced by patients whose CML cells become resistant to the most frequently used anti-CML drug, imatinib (brand name Gleevec).
You will benefit from a bit more information about the concepts discussed in the video.
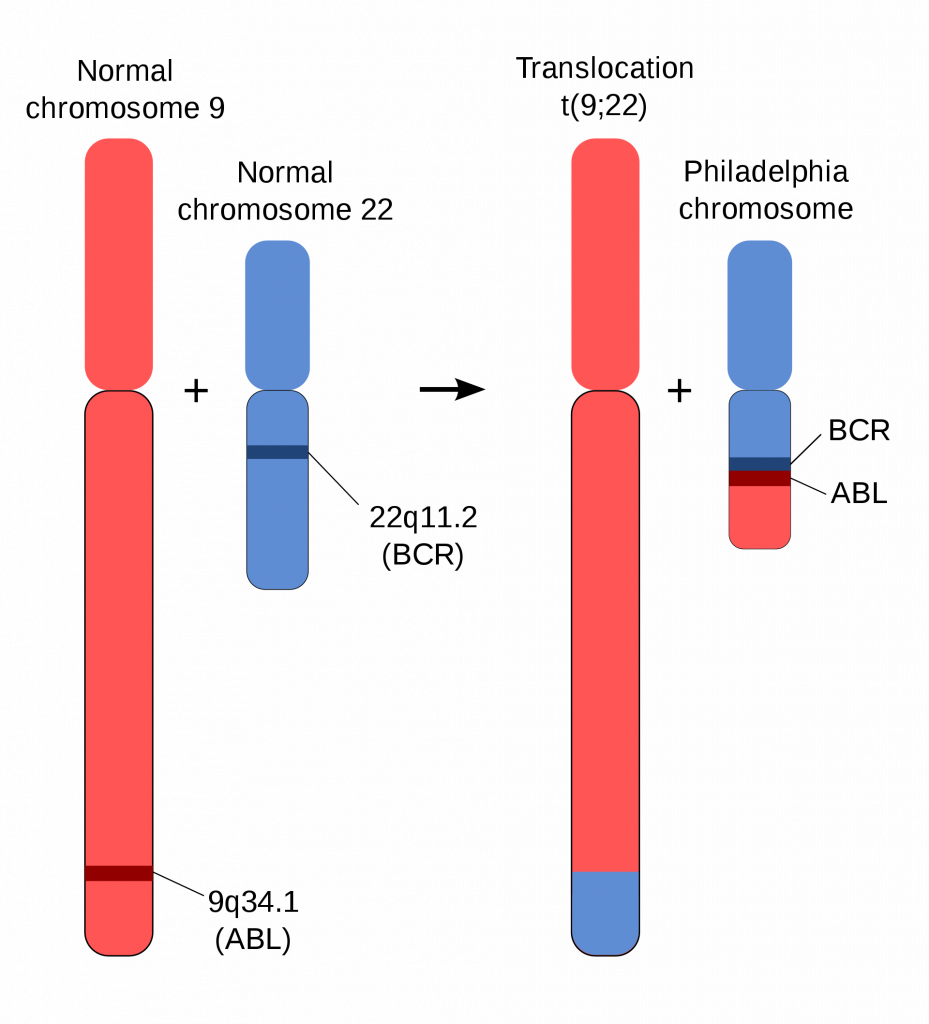
The Philadelphia Chromosome and the BCR-ABL gene
As already mentioned in this text and in the video, the bcr-abl fusion gene causes the common form of CML. The bcr-abl fusion gene is formed when a reciprocal translocation occurs at the cite of the BCR gene on chromosome 22 and the ABL gene on chromosome 9. The bcr-abl gene encodes a constantly active protein tyrosine kinase (PTK) that in turn activates several molecular pathways that contribute to the unregulated growth. The bcr-abl-encoded PTK and the pathways it activates are all potential targets for anti-CML drugs. The chromosome containing the BCR-ABL fusion gene is called the Philadelphia chromosome because the significance of the chromosomal translocation was discovered in Philadelphia. Almost all CML is bcr-abl positive. The few cases that are not bcr-abl are considered atypical. The “demonstration” search and your “final search assignment” search will focus on typical, bcr-abl+ CML.
Bone Marrow and Blood Cells Involved in CML
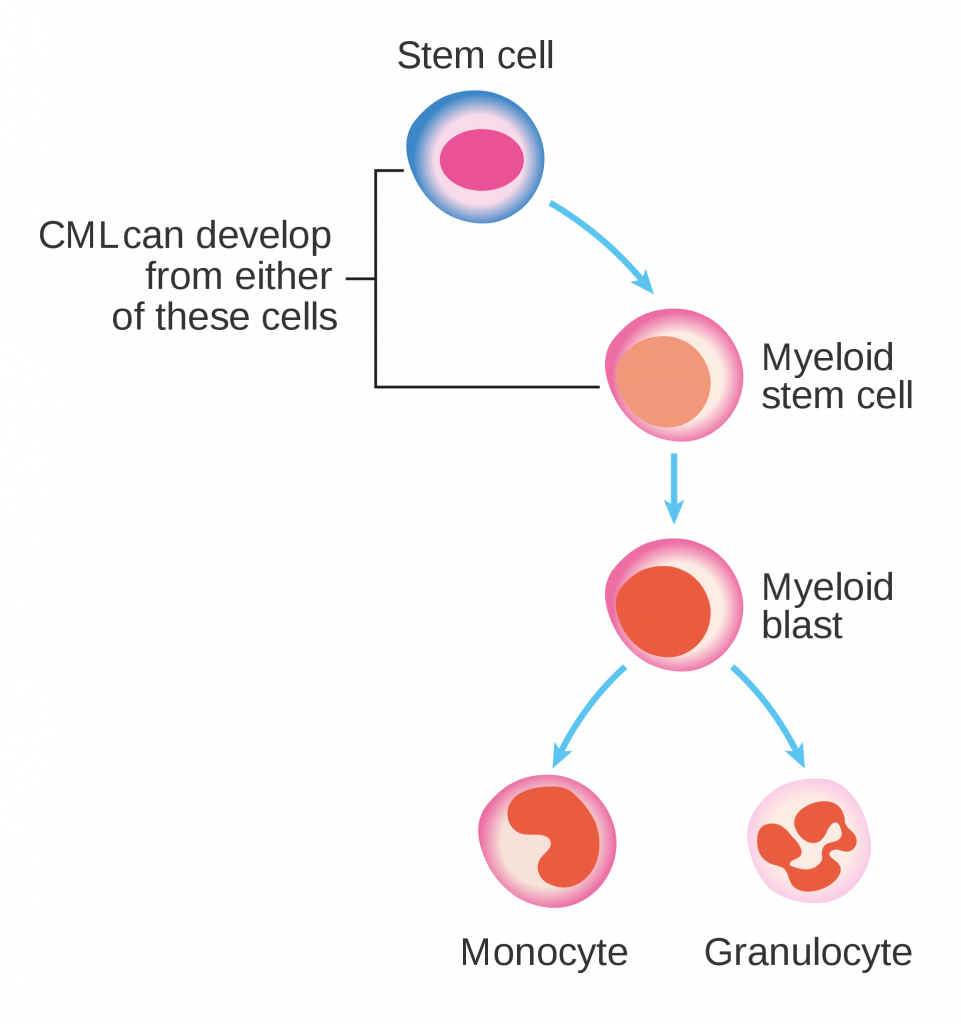
CML may start because of bcr-abl presence in a pluripotent stem cell , a cell capable of replicating itself and producing all blood cell lineages) or bcr-abl activity in a myeloid stem cell (a cell capable of replicating itself and producing all myeloid lineages). The figure below provides a simplified view. There are actually several recognizable stages of cell maturation between the myeloid blast (also known as myeloblast) and the mature granulocyte (neutrophil, eosinophil, basophil) or monocyte.
The additional stages of development are shown in the diagram below.
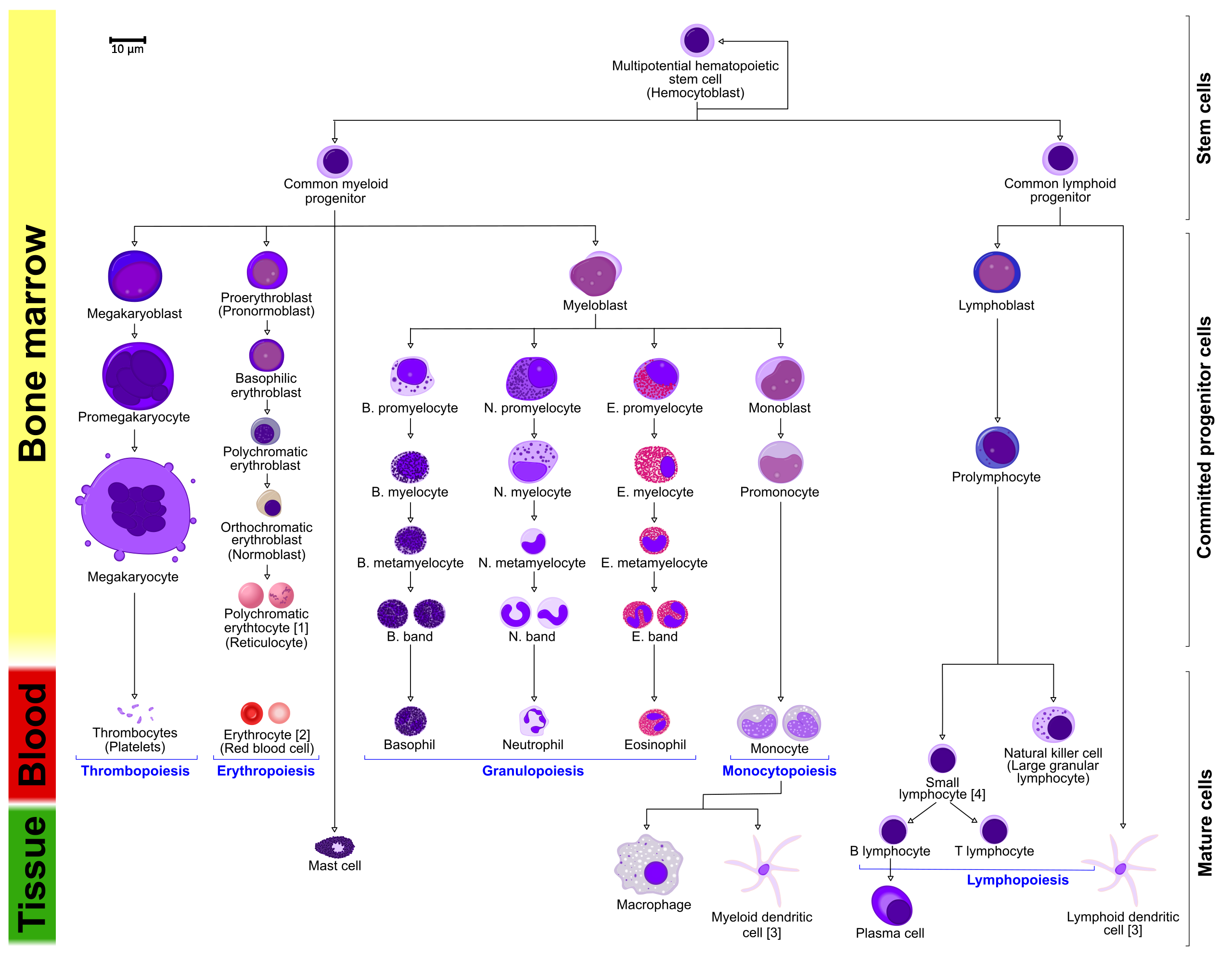
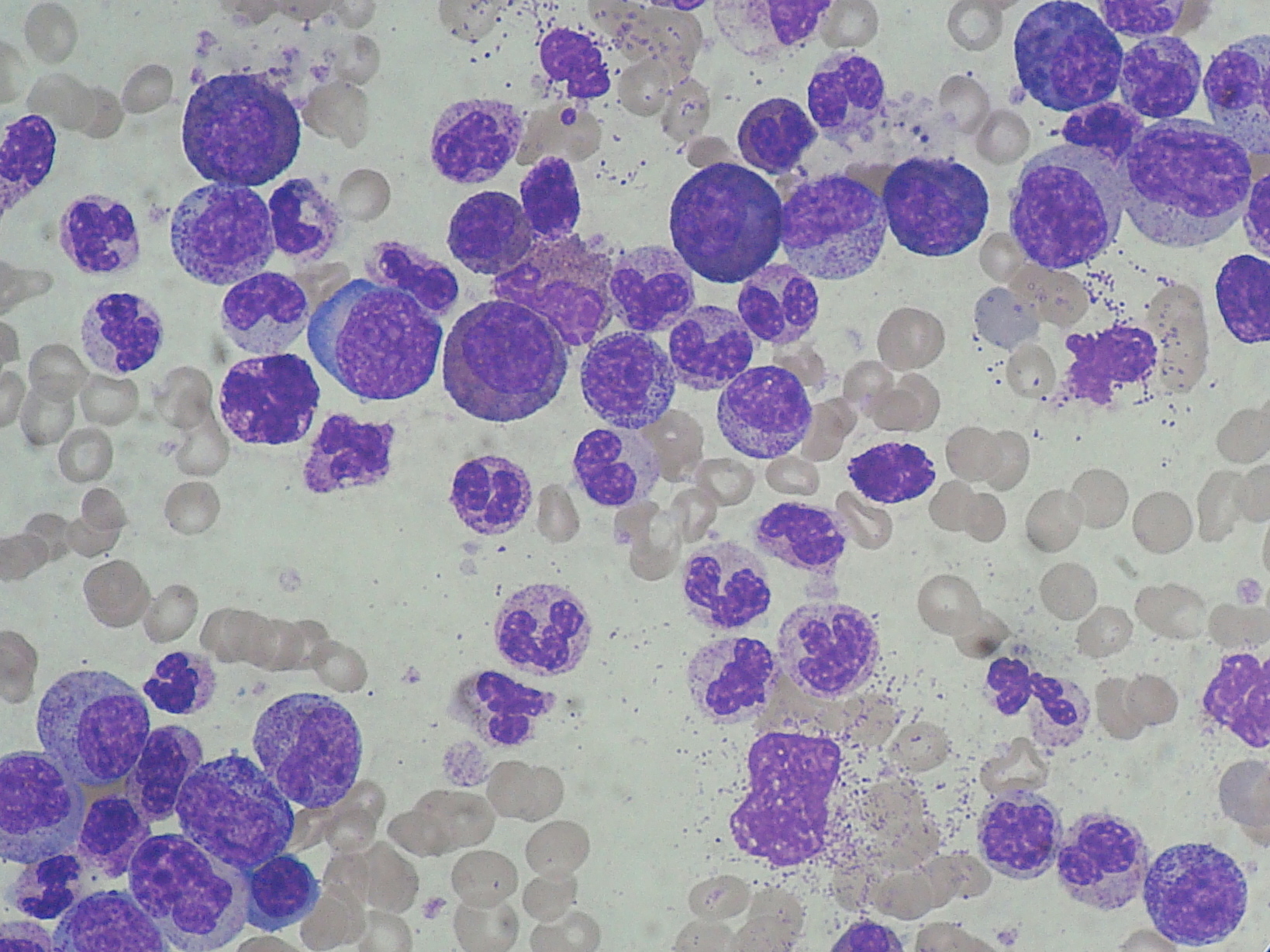
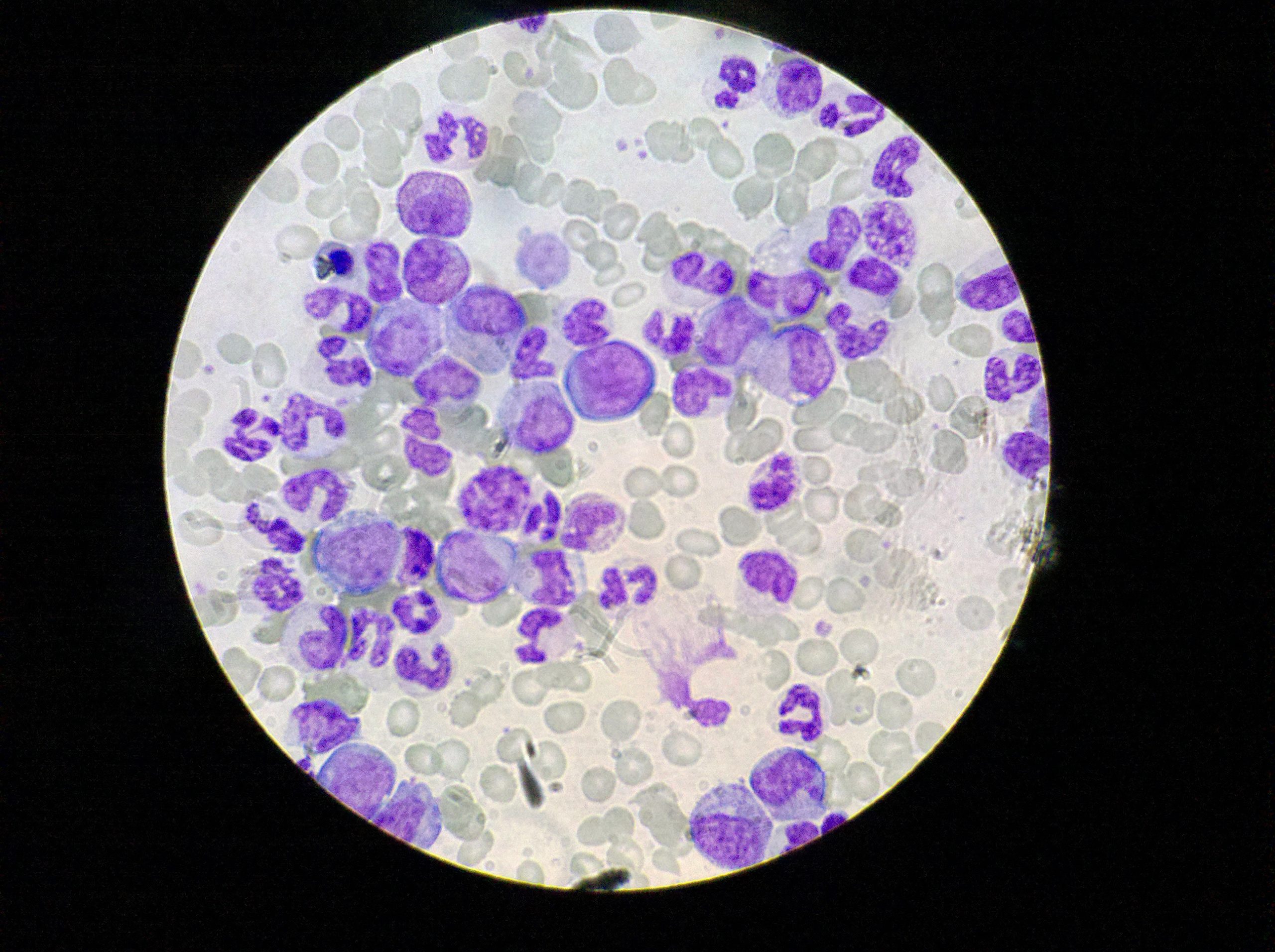
A myeloblast is pictured near the middle of the diagram. All the cell types produced in the myeloblast-containing lineage — myeloblasts, promyelocytes, myelocytes, metamyelocytes, bands and mature cells — can be seen in excess in CML. In normal blood (see figure below), only the mature cells are seen in the peripheral blood.
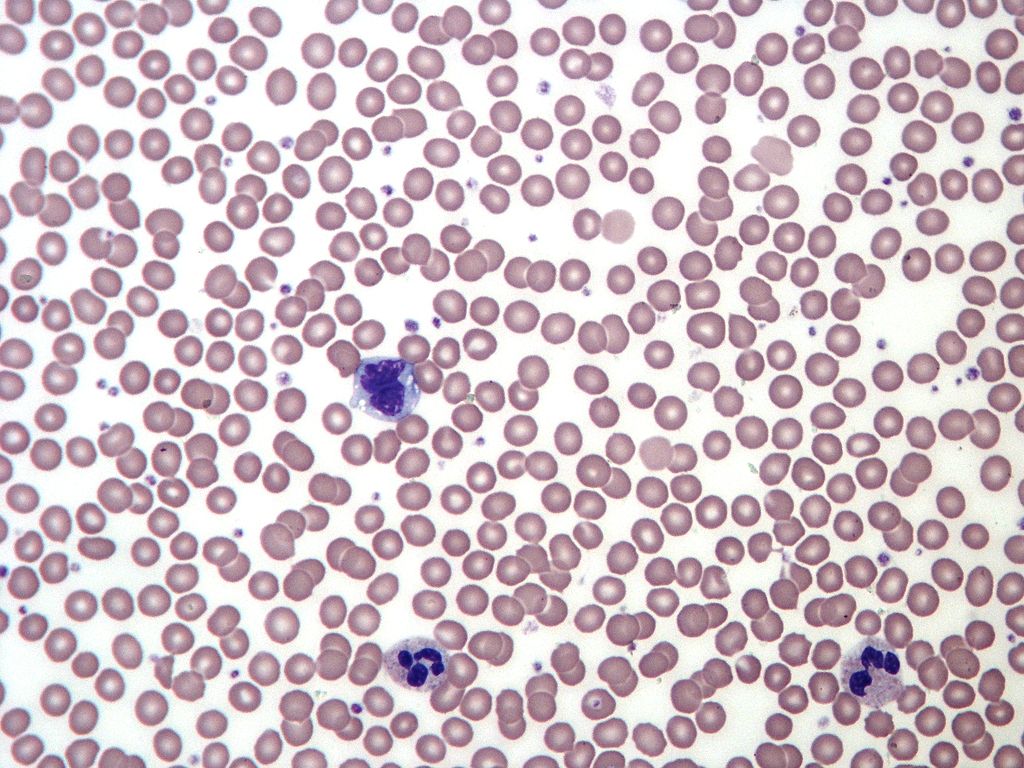
When a healthy individual has a bacterial infection, production of neutrophils ramps up and neutrophil bands may be seen in the peripheral blood. In CML patients, production of myeloblast progeny is so ramped up that all stages of the myeloid lineages can be seen in the periphery (see next two figures below). The neutrophil lineage is most prominent. However, a mild increase in basophils (dark blue granules) and eosinophils (muddy orange-red granules) is present and becomes more prominent if the disease progresses.
Phases of CML
There are three phases of chronic myeloid leukemia.
Phases of CML
| phase | % myeloblasts in peripheral blood white cell count |
| chronic phase CML | < 15% |
| accelerated phase CML (aka transitional phase CML) | 15-30% |
| blast phase CML (aka blast crisis or acute phase CML) | > 30% |
Students often have trouble understanding the idea that CML has phases. I’ve tried to think of an analogy to help you understand.
A person, let’s call him George, is destined to be a serial killer. His life can be seen in three phases. First phase: He starts his life as an abused child who is occasionally mean to others in reaction to the abuse he receives. He isn’t yet making those around him suffer much. Second phase: As he matures, he gains skills in manipulating those around him, he becomes more dangerous, he purposely causes harm to others in his vicinity. Some of those around him begin to experience the unpleasant ‘symptoms’ associated with George’s presence in their lives. Third phase: When he leaves home, all restraints are removed. George can move around freely and begins to kill others.
All three phases of his life are part of George. Just as the chronic phase, accelerated phase, and blast crisis are all part of chronic myeloid leukemia. It would be unusual for someone to mention a phase of George’s life without also using George’s name in the conversation. Similarly, it would be unusual to mention “blast crisis” without saying which disease (CML) is present. Just as CML starts with a long chronic phase that may not cause any symptoms in the patient, George started off with a long period of small angry outbursts or sneaky harms that didn’t cause a lot of trouble to those around him. Like CML then moves into an accelerated phase that often causes symptoms in the patient, George then moved into a period of accelerated ability to manipulate and cause harm to those around him. Finally, like CML then goes into its final killer “blast crisis” phase when the patient usually has symptoms and may die, George moved into his killer phase when he broke free of the restraints he grew up with and began to kill. The accelerated phase and blast crisis of CML can be considered “advanced” disease. It’s harder to treat CML once the disease is advanced. In a similar way, you could call the second phase and third phase of George’s life an advanced stage of his psychopathology. It would be harder to turn his life around and harder to prevent him from harming others once he reaches these phases of his life.
Most CML patients are diagnosed during the early chronic phase of the disease. Many are treated with a tyrosine kinase inhibitor (usually imatinib, also known as Gleevec), respond, continue taking the tyrosine kinase inhibitor, and have no visible disease again.
Some patients have more than 15% myeloblasts in their peripheral blood white cell count at the time of diagnosis. These patients are said to have advanced disease. Advanced disease includes the accelerated phase (15-30% myeloblasts) . Accelerated phase is sometimes called transitional phase. Advanced disease also includes blast phase (>30% myeloblasts). Blast phase is sometimes called the acute phase . Many of the patients with advanced disease at diagnosis still have complete responses to tyrosine kinase inhibitors.
Unfortunately, Some patients fail to respond to tyrosine kinase inhibitors or show signs of disease progression while being treated. These patients are said to have resistant disease (also known as refractory disease). Sometimes another tyrosine kinase inhibitor will work when one has failed.
A patient with advanced disease that responds to treatment has a big decision to make. They have to decide whether they want to continue drug treatment (hoping that it will continue to work) or whether they should try bone marrow transplant. Bone marrow transplant can cure CML but can lead to complications that may be fatal.
Clinical Picture
Up to this point, I’ve talked about the laboratory picture, how the abnormal blood looks in CML. Considering the very abnormal blood picture, it is a little surprising that most patients have no symptoms or just a little fatigue when they are diagnosed. Symptoms (the things the patient notices) are varied. Signs (the things the doctor notes on exam and things seen on lab exams) explain many of the symptoms that are seen.
| Possible Symptoms | Signs |
| No symptoms (asymptomatic) | |
| fatigue, malaise (feel mildly ill) | anemia (low hemoglobin) means that less oxygen is delivered to the tissues |
| weight loss | cancer cell production in the bone marrow consumes calories |
| bleeding episodes | platelets (the blood cells that are central to blood clotting) may be less functional, |
| excessive sweating | |
| abdominal fullness, left upper quadrant pain, feel full after eating very little | 1/2 to 3/4 of patients have an enlarged spleen (abnormal blood cells are consumed by the spleen), The spleen may fill most of the abdomen and press on the stomach. |
| tenderness of the lower breast bone | normal blood cells are crowded out of the normal sites of blood production (pelvis )and other bones become more involved in producing normal blood and/or cancer cells. |
| gouty arthritis | high uric acid levels are seen in the blood of some patients. |
Treatment and Prognosis
The first tyrosine kinase inhibitor developed for CML, imatinib (brand name Gleevec) revolutionized the outlook for CML patients.
| Date | 5 year survival |
| 1993 | 31% |
| 2001 Gleevec approved by FDA | |
| 2001 | 59% |
Many CML patients now have a normal life span on imatinib (Gleevec). Other drugs are used when CML is or becomes resistant (refractory) to imatinib, and some of these other drugs are also being tested as first line treatments (instead of imatinib). One of the drugs used for CML that is not a tyrosine kinase inhibitor is omacetaxine. It is a protein synthesis inhibitor.
As mentioned earlier, the outlook for those who have had imatinib-resistant or advanced CML (accelerated or blast phase CML) is not as rosy as the outlook for those with imatinib-responsive chronic phase CML. Those who have had advanced disease are at greater risk of progression. Bone marrow transplant is an option, but one that carries many risks of its own.
Objective 3. Students will have outlined the major search concepts in the “demonstration” and “final search assignment” searches.
The first step in performing any search is outlining the search concepts.
Major search concepts are the concepts that must be represented with search terms. These concepts usually fall into one of the following categories:
- names of diseases or names of categories of diseases,
- names of drugs/therapies or names of categories of drugs/therapies,
- names of organs or body parts or “wounds and injuries” of named body parts
- names of agents responsible for communicable diseases, names of organisms, or names of animals
- names of infections (Infections caused by a communicable agent and the communicable agent itself are represented by separate headings)
- names of procedures or tests or the names of categories of procedures or tests,
- names of specialties or professions,
- names of specific study designs,
- names of types of programs,
What are the major concepts in the “demonstration” search?
- Does the available evidence support the use of omacetaxine in CML?
What are the major concepts in the “final search assignment” search?
- Does the available evidence support the efficacy of nilotinib in treatment of bcr-abl+, chronic myeloid leukemia that is resistant to another anti-cancer drug?
Objective 4. The sTudent will be aware of the requirements and deadlines for the final search assignment.
Your FSA Topic: Does the available evidence support the efficacy of nilotinib in treatment of bcr-abl+, chronic myeloid leukemia that is resistant to another anti-cancer drug?
1. Dr. Schmidt will demonstrate completion of an FSA on a related topic in class.
2. As you work on the FSA lab assignments, you will create, piece-by-piece, thorough keyword and MeSH, PubMed searches on the topic:
“Does the available evidence support the efficacy of nilotinib in treatment of bcr-abl+, chronic myeloid leukemia that is resistant to another anti-cancer drug?“.
– These will be complicated searches worthy of a librarian or drug information professional.
– You should work individually, but you’re welcome to consult each other.
– You can use relevant portions of the search demonstrated in class.
3. You will troubleshoot and revise searches based on your search results and based on the lessons learned during correction sessions and comments received from Cindy.
– You will work with fellow students to correct each others work.
– You should incorporate the revisions and corrections in the search strategies that you submit as part of your final search assignment.
– Even librarians work with others when producing exhaustive searches. Taking the suggestions of others and incorporating them in your work is an essential part of the final search assignment.
4. You will submit searches for grading in the required template by December 6th. The assignment must be submitted through Canvas. It is worth 50 points.
Required Final search Assignment Template (only use italicized statements if they apply):
Name:__________________
Question: Does the available evidence support the efficacy of nilotinib in treatment of bcr-abl+, chronic myeloid leukemia that is resistant to another anti-cancer drug?
I. Search for MEDLINE records for randomized control trials
A. MeSH
B. Keyword
II. Keyword search for unindexed PubMed records (PREMEDLINE, OLD MEDLINE, PMC)
III. Keyword search for indexed and unindexed PubMed records for systemic reviews
The following drug names were omitted from the keyword search statement because they were used frequently to indicate discussion of irrelevant concepts and were causing retrieval of irrelevant results:
Questions, Problems, Text Errors?
Before you leave, …
- Do you have any questions or do you feel that clarification of some aspect of the materials would be helpful?
- Have you noticed any errors or problems with course materials that you’d like to report?
- Do you have any other comments?
If so, you can submit questions, comments, corrections, and concerns anonymously — or with your e-mail (your choice) — through this online form . Alternatively, you’re always welcome to contact Cindy Schmidt directly 402-650-5056, cmschmidt@unmc.edu, or by making an appointment to meet with Cindy via Zoom.
Answers to questions or requests for clarification that are submitted anonymously will be answered in Canvas on the “Discussions” page for this course.
