
29 Aging Starts Right After Growing Ends
Sabine Zempleni and Sydney Christensen

Image copyright 2013 TheGuardian.com Included under the provisions of fair use under U.S. copyright law.
“Fauja Singh is 102 and is believed to be the world’s oldest runner. Since taking up running, aged 89, he has run nine full marathons. Singh retired from competitive races in February after completing a 10K race in Hong Kong. But he still jogs every day in east London.” The Guardian 2013
Marathon running at the age of 102? Watch Mr. Singh run his last competitive race: https://www.bbc.com/news/av/uk-21565970 .
What allows a person to live a long and healthy life with this level of activity? Why are some seniors able to start running marathons in their 80s, while others are not able to walk up a flight of stairs? Many scientists are interested in the biological mysteries of aging. The ultimate goal of geriatric research is to understand why some people live such a long and active life, then use this knowledge to help others achieve a long quality life as well.
Before we jump in, make sure to review (or learn) previous course material about life-expectancy:
The oldest reported age was 122 years and 164 days, the age at death of Jeanne Calment, a French supercentenarian. This brings up the question: Is there is a natural limit to life? Although the answer is heavily debated by scientists who either align with the “limited” or “limitless” perspective, it is agreed upon that life-expectancy has undergone enormous changes over the last 100 years:
- Since the end of the 19th century life expectancy has immensely increased.
- The number of octogenarians, nonagenarians and centenarians (80-100 year olds) is steadily increasing.
We will start with a couple of definitions.
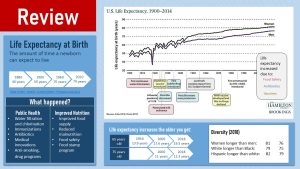
Life expectancy is the average amount of time a person is expected to live given their birth year or period. The most common life expectancy used is the life expectancy at birth, which expresses the average years a newborn infant can expect to live. Keep in mind that this average includes infants who die during the first year of life, young individuals having a car accident, deaths from infectious and chronic diseases and so on. If the infant mortality due to infectious diseases or wars is high in a country the life expectancy at birth declines. If a pandemic, infectious or non-infectious, impacts a population the life expectancy will decline.
In addition to the life expectancy at birth, we can also look at the life expectancy for 65 or 75 year old adults. This will allow us to understand how long a 65 year old person can expect to live after surviving childhood diseases, accident prone teen and young adult years, and middle age with early heart attacks.
Over the last 150 years, the life expectancy at birth in the US rose from an average of 40 years to an average of almost 80 years today. If you look at the life expectancy graph above, you also see that since the 1950s, life expectancy has steadily risen without much fluctuation.
By the way, the deep dip in 1918 reflects the impact of the Spanish flu pandemic; we see a dip stemming from the COVID-19 pandemic when millions of people died as well.
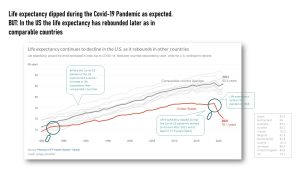 The COVID-19 pandemic dip: The statistics are in. As expected we saw a dip in life expectancy in 2020 related to the huge number of COVID-19 deaths. This was expected based on the 1918 flu pandemic data which featured a similar dip. During a pandemic many people die, and this impacts the life expectancy of the infants born during those years. At this point, US researchers are ringing the alarm bells though. While other comparable countries recovered from the dip in life expectancy, the US life expectancy kept steeply declining until 2021. Good news, in 2022 life expectancy increased by 1.1 years to 77.6 which is still lower than comparable countries. Here is the article: https://www.npr.org/sections/health-shots/2023/03/25/1164819944/live-free-and-die-the-sad-state-of-u-s-life-expectancy
The COVID-19 pandemic dip: The statistics are in. As expected we saw a dip in life expectancy in 2020 related to the huge number of COVID-19 deaths. This was expected based on the 1918 flu pandemic data which featured a similar dip. During a pandemic many people die, and this impacts the life expectancy of the infants born during those years. At this point, US researchers are ringing the alarm bells though. While other comparable countries recovered from the dip in life expectancy, the US life expectancy kept steeply declining until 2021. Good news, in 2022 life expectancy increased by 1.1 years to 77.6 which is still lower than comparable countries. Here is the article: https://www.npr.org/sections/health-shots/2023/03/25/1164819944/live-free-and-die-the-sad-state-of-u-s-life-expectancy
The question is now: what contributes to the steady and smooth rise in life expectancy?
Amazing medical innovations during the 20th century are the major contributors. On the forefront are the development of vaccines and antibiotics that reduced the mortality of children and adults alike. Before the discovery of vaccines and antibiotics, infectious diseases were the top cause of death. A simple cold, the flu, or any other infectious disease could cause death at any time during life. Many children died due to diseases most of today’s parents are not familiar with: Polio, measles, mumps, rubella, diphtheria, tetanus and pertussis. Pandemics of those diseases kept racing in waves through schools leaving death and disability behind. Before some parents started refusing childhood vaccinations, these dangerous diseases were almost eradicated. In recent years the prevelance of those socalled childhood diseases are on the rise again.
New medical procedures and drug development expand life today. Even if a person develops a non-communicable diseases they have a good chance to live with this disease to old age.
Improved hygiene (personal, medical, and food safety) prevents the spread of communicable diseases. The chlorination of water stopped epidemics of gastrointestinal diseases in industrialized countries almost completely.
The other big factor is improved nutrition. Our food system not only became safer, but food became cheaper and more widely available. Social programs such as SNAP (formerly food stamps) ensure that people living in poverty will not starve to death.
If you ever have some time, I recommend reading The Jungle (1906) by Upton Sinclair, an American journalist and novelist. He went undercover in the Chicago stockyards to describe the harsh conditions and exploited lives of immigrants in Chicago. You will also learn a lot about the food production system back then. I only made it 3/4 through the book because the conditions described were so horrible that I could not take it any longer!
When looking at the life expectancy for 65 and 75 year olds we see a continued increase during the last decades. This is absolutely amazing! Unfortunately, this is not the case for everyone:
Equity: There are disparities in life expectancy associated with both race and sex. The life expectancy at birth is 6 years higher for white Americans than Black Americans. We have previously discussed this diversity issue; recall that Black Americans suffer more from T2D and other chronic diseases, as well as maternal mortality. Women live longer than men.
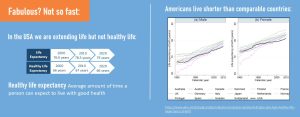
Comparison to other countries: The life expectancy in the US might be high, but it is not exceptional. Other industrialized countries make more progress (see graph above).
Healthy life expectancy: Long life is not enjoyable if the quality of life is low, thus the healthy life expectancy takes the years of ill health into account. It is the average amount of years in good health a person can expect at birth. The average in the US is approximately 66 years, and hasn’t increased in the last two decades. This gap of 13 years is the reason why many seniors live their last years with a low quality of life.
You Will Learn:
1. Aging is the gradual, progressive loss of physiological function over a lifetime.
- Biologically, an adult is defined by having reached physical maturity. Physical maturity includes that growth is mostly completed and sexual maturity is reached.
- There are several categories of adults: Young adulthood, middle adulthood, older adulthood.
2. The onset and acceleration of the aging process varies widely.
3. Effective age can be estimated taking chronic disease symptoms into account.
Aging is the Gradual, Progressive Loss of Physiological Function Over a Lifetime
Becoming an adult has several dimensions: biological, psychological, and social. From the standpoint of nutrition sciences, we are mostly interested in the biological dimension.
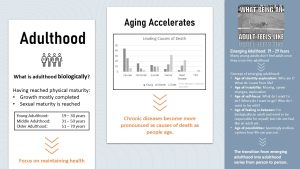
Biologically, an adult is defined as having reached physical maturity: The point at which growth is mostly completed and sexual maturity is reached.
This simple definition would include everybody from 19 to 120 years old, and we can all agree that a 19 year old is very different from a 120 year old. Once we reach adulthood, our bodies do not remain in the same physiological state for the rest of our life. While we will not grow and physiologically mature anymore, there are still many physiological changes occurring.
This is why we subdivide adulthood into three general age groups:
- Young adulthood: 19 – 30 years old
- Middle adulthood: 31 – 50 years old
- Older adulthood: 51 – 70 years old
Keep in mind that this is a very rough definition. You will later learn that for many people the chronological age does not necessarily match the physiological age.
Young adulthood: the time when our body is physiologically at its peak: peak bone density is reached, lean body mass is highest, metabolic processes tend to run flawlessly. Aging processes are present, but not noticeable.
Emerging Adulthood: Notice that the biological definition does not fully describe this age group. When we look at young adults from a socio-psychological standpoint, it is clear that being an adult is not as easy as reaching the age threshold of 19 years. Many 19 year olds start college and certainly do not feel like an adult. This phase in life can be described as emerging adulthood: a time of identity exploration marked by instability and self-focus. Although most young adults feel in-between childhood and adulthood, the timing when young people transition into adulthood and feel like an adult can greatly vary.
Middle adulthood: After age 30, the aging process is ongoing, but is only barely noticeable in healthy adults living a healthy, active lifestyle .
Older adulthood: Age 50 is usually the time when aging starts to become more noticeable. People notice their age, even if they are healthy and fit. Joints become stiffer and achy, weight becomes much harder to maintain. If the person has had an unhealthy lifestyle, symptoms of chronic diseases start showing.
The image depicting the leading causes of death (middle of the infographic above) illustrates that aging tends to speed up in later life.
The main causes of death for young adults are injuries, followed by homicides and suicides. Chronic diseases play only a minor role. As we age, the causes of death are more influenced by the aging process and lifestyle—shifting towards cancer and heart disease—especially in older adults.
You might have noticed that the adulthood definition only reaches until the age of 70. Is everybody above just old and not an adult anymore?
Next Question: What Is Old?
Old people are often separated from older adults because they start having different needs. Of course they are still adults! You will learn about high age later in chapter 31, 32, and 33. For teens and young adults, being old seems to start at middle age, sometimes even earlier. This is then countered by remarks such as 50 is the new 30. For the sake of this course, we will use the scientific definition though.
The Onset and Acceleration of the Aging Process Varies Widely
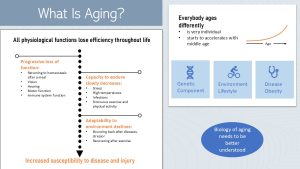
First, here is the bad news: all physiological functions lose efficiency throughout life. And yes, that process starts right away once growth and physiological maturation is completed.
During growth, tissue is built and modified; however, once growth and maturation is completed, the focus shifts to maintenance of tissue.
After many years of cell divisions due to tissue growth and maintenance, cells start aging. This in turn triggers loss of some organ and tissue function.
The good news is that initially this is a slow process. Once older adulthood is reached, the wear and tear starts to speed up slowly, and reaches the fastest acceleration in the senior years.
Some loss of efficiency and adaptability is clearly visible: the need for reading glasses, having trouble seeing at night while driving, getting less flexible, and some loss of strength. Does that describe your parents and grandparents?
Other changes are less visible:
- Our immune system will age, and immune cells will not fight off pathogens as easily. Many older people—not all though—are sick more often and tend to experience communicable diseases such as the flu or cold more severely.
- After eating, returning to homeostasis takes longer which increases the risk for developing for example T2D.
- Other systems become less able to endure the environment we are living in. Ask any aging adult and they will tell you that while they can deal with stress, high temperatures, or strenuous exercising, it becomes increasingly harder to bounce back afterwards.
- Declining function and decreasing capacity to endure stressors increase the risk for disease and injury with age.
What is returning to homeostasis after a meal?
When we start a meal, the smell and taste of food triggers neurological and hormonal signals to get our body ready for digestion. Once eating starts, an array of digestive and metabolic processes are started:
- Mouth: Taste receptors and the somatosensory system signal incoming food type. Digestive enzyme production increases depending on the detected macronutrients. Gastric juice production and GI motility also increase.
- Stomach: Stretch receptors regulate intake of food amount and short-term satiety
- Small intestine: Receptors provide information about nutrient composition of food and activate appropriate metabolic pathways. Stretch receptors provide information about amount.
- Metabolism: Presence of nutrients in the blood circulation and cells modulate metabolic pathways.
Once all nutrients are metabolized or stored, this machinery goes back to normal, which is called returning to homeostasis. Slower return to homeostasis makes us more vulnerable for chronic diseases. For example, blood glucose levels stay elevated longer, increasing the risk for T2D.
Effective Age Can Be Estimated Taking Chronic Disease Symptoms Into Account
It would be great if we knew how well we age. If it turns out we age at the faster side it would be fantastic if we could receive some sort of treatment to slow down aging. While science is not anywhere close to providing treatment for aging, scientists have developed the concept of the “effective age” based on what we know today about the aging process.
Even in healthy individuals, the risk for age-related chronic diseases such as cancer, T2D, CVD, Alzheimer’s, dementia, or reduced cognition increases due to cellular aging processes. More details about cellular aging later.
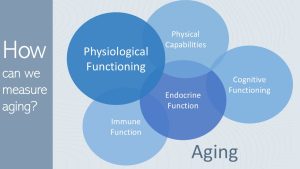
This brings up the question how scientists research the complex concept of aging. In order to gain a better understanding, aging is broken up into several components:
- Physical capabilities: Describes the appearance of an adult. How much strength does the person have? Does the person function in daily life without undue effort? Only partially? Is the person still able to exercise intensely?
- Physiological functioning: Determined by running lab tests on blood and urine, physiological functioning describes the biophysical and biochemical processes, homeostatic control mechanisms, and communication between cells.
- Endocrine function: Part of physiological functioning, and describes changes in hormone secretion and interaction (for example: HPG axis, HPA axis, insulin secretion).
- Immune Functioning: Ability of the immune system to work in a balanced way, including chronic systemic inflammation as well as the ability to identify and remove threats efficiently.
- Cognitive functioning: Includes everything from mild cognitive decline (forgetting things, less ability to focus, learn or memorize) to the development of dementia and Alzheimer’s disease.
Some of the aging processes I just described are unavoidable. They are promoted by wear and tear as well as genetic predisposition. During the next chapters, you will learn about the physiological and molecular aging processes, including how chronic diseases accelerate aging processes.
Individual differences are determined in part by genetic predisposition, but lifestyle choice is another much larger factor. Developing chronic diseases early due to an unhealthy lifestyle speeds up aging, reduces quality of life, and hastens death.
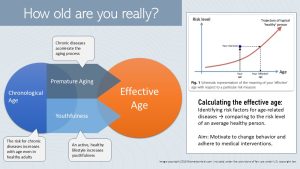
This is how the concept of the efective or biological age was developed. Effective age tries to calculate the true age based on risk factors for chronic diseases. Mathematical calculations collect the risk factors, calculate a risk level, and plot the risk level against the chronological age.
Based on scientific data, the red curve depicts the relationship between risk level and chronological age in healthy adults. Using this curve, this risk level is extrapolated (see infographic above, upper right side) to the biological/effective age. If the risk level is low, the effective age is lower than the chronological age. If the risk level is high, the effective age is higher than the chronological age.
This concept could be used to design personalized health care, but at this point in time the science is not precise enough. Currently, the primary purpose of the effective or biological age is to generate awareness.
Editor: Sydney Christensen, Meryn Potts
NUTR251 Contributors:
- Spring 2020: Ericka Knapp, Brittany Southall, Miranda Haverdink, Kennedie Engles, Krissy Krager, Kendyl Heuertz
- Fall 2020: Bryson Krull, Kaitlyn Higgins, Morgan McCain, Collin Mahler
A person who has reached the age of 110.
A disease that is not transmissible from person to person. NCDs include CVD, cancer T2D, hypertension, dementia, addiction to name just a few.
Illnesses that spread from person to person.

Feedback/Errata